
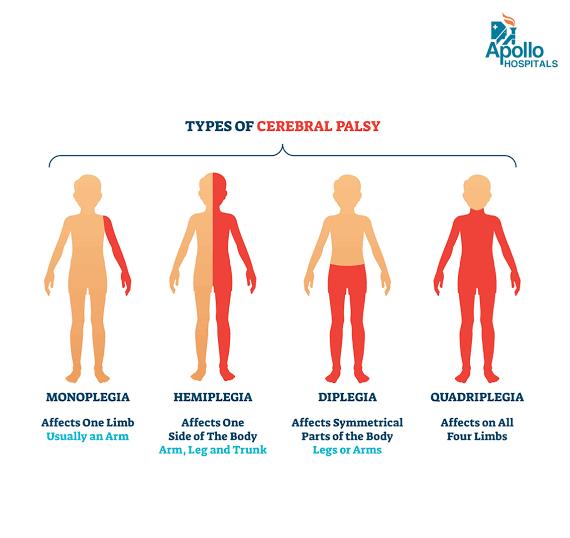
Types Of Cerebral Palsy
Abnormality of movements in cerebral palsy
This is the result of disturbance in the lower motor neuron. The muscle or group of muscles affected may be totally paralyzed If all their available neurons are put out of action. If only some anterior horn neurons are involved the muscles will show partial paralysis and will appear to be very weak. Any muscles affected in this way would be unable to function as members of a team and consequently movement synergies requiring their participation would be abnormal and substitute patterns would be produced.
If only a small muscle group is affected in this way the abnormalities are minimal, but if many groups are involved, substitution can be grotesque or even inadequate, in which case the subject is rendered relatively helpless.
Totally flaccid muscles have no lower motor neuron supply because of damage or injury to all the cells in their motoneuron pools or to all the fibers passing peripherally. Such muscles cannot be brought into action voluntarily, or as an automatic reaction or in a reflex action. They feel soft and flabby to the touch, are non-resilient, offer no protection to the structures adjacent to them and are unable to support the joints over which they pull. Because of lack of use, and therefore of blood supply, they atrophy quite rapidly losing the greater part of their muscle bulk.
2. Hypotonia
This term is used here to denote the reduction in preparedness for action found in the muscles when there are defects in certain areas of the extrapyramidal part of the central nervous system. In this case the excitatory influence exerted by the extrapyramidal system upon the motoneuron pools is diminished and, as a result, the muscles show a reduction in sensitivity to stretch. This may, at first sight, be confused with muscle paralysis because the muscles may appear to be totally or almost totally flail. It is, however, very different. The muscles have a normal lower motor neuron supply but the factors exerting an influence upon the motoneuron pools are seriously disturbed. There is a reduction of excitatory influence upon the small anterior horn cells which give rise to the fusimotor fibers. Because of this the fusimotor fibres are inactive and therefore activity of the intrafusal muscle fibres is diminished. Thus the muscles are less sensitive to stretch.
3. Ataxia
A patient who has hypotonia also shows a form of ataxia.
The symptoms described under the heading 'hypotonia' are also those of ataxia.
Ataxia means that movements are incoordinate and ill-timed, giving a deficiency of smoothness of movement.
Ataxia related to hypotonia occurs partly because of the defective postural tone as a background and partly because of the phenomenon of dyssynergia.
Dyssynergia is the term used to describe the loss of fluency in a movement. The balance of activity is upset because of faulty synergy. The teamwork between muscles is lost, giving a jerky appearance to the movements, which may well be split up into a series of jerky, separated entities. Both stopping and starting of movements are difficult and overshooting occurs.
These symptoms may also be noted when hearing a patient speak. Speech is a very mature ability, requiring control and co-ordination of the appropriate muscles. Dyssynergia and accompanying problems lead to speech being broken up in the same way as was described for movement. Speech affected in this way is said to be 'scanning'.
It may be due to deficiency of afferent information to the cerebellum and to the cortex, making the individual unaware of his position in space. In this case the cerebellum cannot bring about the necessary postural adjustments, nor is the central nervous system receiving a feedback regarding the success of the movement. A person with this problem will show very similar symptoms to the previous form of ataxia, but he may be able to mask his problem by using his eyes and ears to excess as substitutes for his loss of skin and joint position sensation. If he is temporarily deprived of the use of his eyes - as in the dark - or of his ears - as in a noisy environment - he may be much more ataxic than when he is able to make full use of them.
The ataxias are often accompanied by nystagmus, which is a form of dyssynergia in the eyes.
Occasionally ataxia may be accompanied by vestibular disturbance which gives rise to vertigo. This is a condition in which the patient's appreciation of head position is disorientated. The subject feels giddy and nauseated. These symptoms can add greatly to the problems of the ataxic patient.
Dysmetria is a term often applied to the ataxic patient. It refers to the difficulty in assessing and achieving the correct distance or range of movement.
4. Hypertonia
This denotes the opposite state of affairs to hypotonia. There are two types of hypertonia, spasticity and rigidity.
As was stated before, the fusimotor system is excessively active. The sensitivity of the stretch receptors is excessively high to both slow and quick stretch stimuli.
Spastic patterning varies from moment to moment depending upon many factors. One factor is the general position of the patient. Another is the nature of the stimulus being applied to the patient and yet another is how much effort the patient is making to obtain a voluntary movement. Strong volition often simply facilitates the excitation of the spastic patterning. This is possibly because the threshold of the appropriate motoneuron pool is already low, due to reflex release, so that the slightest volitional effort triggers them into action.
If the damage to the central nervous system is lower in level so that only the spinal reflexes are released then the spastic patterning may well be more related to flexion withdrawal. According to the stimulus applied there may be flexion or extension patterning but flexion is more likely to be predominant. Withdrawal is a response to noxious stimuli, but in this type of case it can be the response to almost any stimulus: touching of bedclothes on the affected areas, vibration, noise, sudden movement.
It is well to bear this in mind since such patients must be dealt with very carefully if flexion withdrawal is not to become a permanent position for the patient.
Spasticity is never isolated to one muscle group. It is always part of a total flexion or total extension synergy. Let us take a lower limb example. If the lower limb is in extensor spasticity it will tend to adopt hip extension, adduction and medial rotation, knee extension and foot plantar flexion. Thus if one detected spasticity in the adductor groups one should expect it in all the other groups in the pattern.
It should be noted that the limb is not put into a good weight-bearing position by this patterning. The heel is unable to touch the supporting surface and the adducted limb is unable to support the pelvis adequately. Thus the patient showing this patterning is not able to experience the appropriate stimuli which will give the slow-acting postural muscles the appropriate guidance to support the limb.
For sound supporting posture we require the normal afferent stimulus of compression upon the heel of the foot. In this way the appropriate malleable postural mechanisms giving balanced co-contraction of both flexors and extensors can be encouraged.
If this occurs we do not show the hyperextended knee of the mildly spastic or the complete inability to get the heel on to the ground of the severely spastic case.
The spastic patient of this type may be deprived of experiencing the very afferent stimulation which could make his postural tone more normal. This occurs in many ways to the patient with this abnormal patterning and is an important factor in his treatment. The physiotherapist must help the patient to experience afferent stimulation which he is, by his condition, denied.
Reflex release mechanisms are more often than not incomplete.
In this type of hypertonicity the fusimotor system is also excessively active giving an increase in sensitivity to the stretch receptors in muscle. The disturbance is thought to lie at a different level from that causing spasticity since there is a considerable difference in the type of change in response to stretch.
It will be remembered that the subcortical nuclei comprising the basal ganglia are thought to help in the production of postural fixation by exerting their influence upon the stretch reflex mechanism via the reticular formation. They help to maintain adequate postural fixation while allowing the necessary malleability for voluntary movement.
In rigidity the muscles respond to slow stretch by steady resistance which does not particularly build up or relax off. There is a tremor which is said to give a 'cog-wheel' effect, or the limbs may feel like lead when moved, giving rise to the term 'lead-pipe' rigidity.
Patients showing rigidity usually have lesions in the subcortical areas and show a typical posture which becomes progressively more flexed. They do not rotate in any of their movements and lack of axial rotation seriously interferes with balance reactions.
The 'rigidity' patient shows movement problems in which automatic adjustment and activities do not occur freely and therefore voluntary movement is slow and impoverished because it is unaccompanied by automatic balance reactions and because it occurs so slowly against the ever-resisting stretch mechanisms.
5. Athetosis
When this occurs the patient shows disorder of movement because of fluctuation in the level of postural fixation. The patient adopts a succession of abnormal postures which may be quite grotesque. The condition is made more severe by excitement and emotional stress. It is thought to be due to lesions within the basal ganglia. In this instance the basal ganglia are failing in their ability to encourage adequate postural fixation and fluctuations therefore occur.
Involuntary movements occasionally occur but the symptoms are always made worse by voluntary activity.
6. Choreiform activity
This is a series of involuntary movements, which occur in the face and limbs. They are quicker than those of athetosis and are also made worse by voluntary movement. Many patients show a combination of choreiform and athetoid activities. The basal ganglia are considered to be at fault in choreiform problems.
7. Ballismus
This is a term used to describe wild flinging movements which may occur to such an extent that they throw the patient off balance. The condition usually occurs as a result of a lesion in the subthalamic region and only affects one side. In this case it is called hemiballismus.
8. Dystonia
This is a term used to describe an increase in muscle tone that is antagonistic to the intended movement. The symptoms tend to prevent movement and may pull the individual into grotesque postures. It may affect one part of the body or the body as a whole. Spasmodic torticollis is thought to be a type of local dystonia.
